 |
THE INSULIN TREATMENT OF SCHIZOPHRENIAFrom An Introduction to Physical Methods of Treatment in Psychiatry (First Edition) by William Sargant and Eliot Slater (1944, Edinburgh, E & S Livingstone). |
| Not long after insulin came to
be generally used in medicine it was found that in small doses it could be used to improve appetite in cases of anorexia, and that there followed a general improvement in the physical and mental state. The clue was not followed up until Sakel came to use insulin hypoglycaemia to counter the symptoms of withdrawal in the treatment of morphine addiction. He found that he got the best results when a sufficient dosage of insulin was given to produce clinical hypoglycemia, and that this phenomenon, hitherto considered dangerous, was readily controlled by the administration of sugar, when the patients were watched throughout. He was led to try its use in the I treatment of schizophrenia, and the Vienna Clinic, which had seen the first introduction of the malarial treatment of general paralysis, provided him with the patients to experiment on. The idea seemed bizarre, but it was found to work. Once tried its results were, in individual patients, so surprisingly favourable that its use spread widely and quickly. In the international congress of 1938 reports were presented of its trial in most of the civilised countries of the world; nearly all of them were favourable. The disorganisation of the war years has to a great extent interrupted its progress in England but it has gone ahead much faster in America. |
Manfred Sakel |

STATISTICAL RESULTS
Reliable statistics are mostly
in favour of the value of the
treatment. In a series of over 400 patients
treated in Swiss
hospitals before 1937, when the technique was still
new,
59 per cent. of persons treated within the first six months
after
onset reached either a complete or social remission. In
the New York State
hospitals of over a thousand schizo-
phrenics treated with insulin 11.1 per
cent. recovered, 26.5
per cent. made great improvement, and 26 per cent.
some
improvement; the corresponding figures in over a thousand
control
patients were 3.5 per cent., 11.2 per cent. and 7.4 per
cent. A comparable
number of patients treated with cardiazol
convulsion therapy did not do even
as well as the control
patients. Furthermore, the treatment greatly shortens
the
duration of the illness. Earl Bond reports that in the Penn-
sylvania
Hospital 95 per cent, of the patients who were
treated and recovered left the
hospital within a month of
termination of treatment; with few exceptions the
un-
treated patients who made spontaneous remissions required
one to three
years for a similar improvement. Thirty-eight
per cent. of his treated
patients remitted, where there had
been previously only 10 per cent,
remission and 10 per cent
improvements occurring spontaneously.
The results are much more
favourable when treatment is
given early. The New York State hospital figures
show that
only 27 per cent. of the patients treated in the first six
months
of the illness failed to improve, whereas this figure rose to
66
per cent. for those whose illness had lasted five years
Taking a dividing
line of 18 months, Earl Bond finds 67 per
cent, recovery and great
improvement with treatment given
before that time after onset, 30 per cent.
after. The prog
nostically favourable patients selected for admission to
the
Maudsley Hospital showed 34.5 per cent. of social recoveries
when
followed up for three years; 70 per cent, of the patients
selected for
insulin treatment recovered in the same hospital
at a later time. In both
these groups the illness had not
lasted longer than a year.
It is not yet known whether
these recoveries will be maintained;
but the three to one ratio in frequency of
improvement in treated
as compared with untreated schizophrenics
quoted
from the New York State hospitals statistics was still
maintained after two
years, and 60 per cent. of the insulin
treated patients were still living in
the community mostly
in a recovered or improved condition. Relapses occur
both in
patients who have recovered spontaneously and with insulin
It may
be that as the years progress treated and control
groups will tend to
approximate; but even if this proves
to be true one would wish to keep the
potential lunatic sane
as long as possible, and to give him as long a period
as
possible of health and happiness. There is also evidence
that the
relapsed schizophrenic is still susceptible to
treatment especially if each
relapse is treated immediately it
starts.
Provided early cases are
treated, it is then probably true
to say that insulin treatment brings about
a remission quicker
and in a higher proportion of patients than occurs
spon-
taneously or with convulsive therapy. There is also a less
unanimous
impression that the quality of the remission
obtained with insulin is better
than that of the spontaneous
remission; this is likely to be true, if for no
other reason than
that recovery takes place earlier under treatment and there
is
less time for the psychological scarring that is the most
terrible
effect of the disease. There is unanimity that in the
earliest months of the
illness the results are out of all pro-
portion better than later on. In some
patients the illness
comes on so insidiously that even retrospectively none
but
the widest limits can be assigned to the time when it started,
and
these patients it is generally agreed are the most un-
favourable
therapeutically. This may quite possibly be not
because the form of the
illness is more malignantordinary
clinical judgment suggests the opposite
conclusionbut
because in all these patients the illness is likely~ to have
lasted
for months or even years before it is even suspected.
Finally, it is clear that there
is an art of treatment, in which
some will be more adept than others, and
that operations
cannot be conducted by rule of thumb. Different
workers
have obtained very different results with the same type
of
material, both in the frequency of remission and of
unpleasant
complications. Earl Bond notes that in a group treated in
the
Pennsylvania Hospital between 1936 and 1938 treatment
was given tentatively
and was in the hands of several different
physicians and all possible risks
were avoided; only 46 per
cent. of remissions was obtained in cases of less
than a years
duration. After 1938 a single skilled therapist was
employed,
and the comparable remission rate rose to 79 per cent. This
may
be partly because where there is a specific treatment
available, patients
still in the early stages of the illness are
encouraged to seek treatment;
but at least part of the im-
provement in the recovery rate must be
attributed to the
greater expertness of the treatment and the giving of
really
deep comas when necessary. It is only too easy to carry out
the
treatment in a slipshod or incautious way, or to err on the
side of over-easy
discouragement. The successful therapist
will be gifted with enthusiasm and
caution, he will have a
sympathetic interest in and a detached appreciation
of the
personalities of his patients, he will have the general
medical
training that has accustomed him to the handling of
medical
emergencies, and the refined clinical judgment of the
èx-
perienced psychiatrist, and he will have the facilities to give
the
whole of his energy to the treatment of his patients
without administrative
after-thought. The abilities of the
therapist are not less important than the
method of treat-
ment adopted. On his skill alone the recovery of any
particular
patient may ultimately depend.
THE SELECTION OF
PATIENTS
It is rarely indeed that
facilities will exist for the treatment
by a full course of insulin of all
the schizophrenics coming
under observation, and it is therefore important
not to waste
the treatment on patients not very likely to respond
while
denying it to the favourable case. The first point for
considera-
tion is the length of duration of the illness, and this does
not
mean of overt symptoms. The patient who has only recently
come to show
definite and unmistakable symptoms but has
been known to have been gradually
becoming queerer for
several years is not a favourable case for treatment.
The most
favourable case would be the patient who had been well up
to a
few days or weeks of being seen, and he should be selected
even if there is
some lingering doubt of the true nature of the
illness and probabilities only
speak in favour of schizophrenia.
An atypical onset should not be allowed to
develop gradually
over the course of months into an unmistakable
clinical
picture before treatment is begun. This position is likely
to
arise in atypical manic excitements, in obscure confusional
states, and
even in depressive states with a suggestion of
catatonia, of hallucinations
or other suggestive symptoms. In
any case it must be remembered that
schizophrenic psychoses
greatly outnumber all others in persons under the age
of
thirty. From the much greater success in the early case it
follows that
once treatment is decided on it should be begun
at the earliest possible
moment. If there is a waiting list for
admission, the early schizophrenic
should take precedence of
most other patients, firstly for the reason
already given, and
secondly because in the early stages the clinical picture
is
very fluid and an attempted suicide, an attack of excitement
or
violence may remove the patient from the possibility of
treatment where it
has been arranged to another place where
there may be further delays. As even
a few weeks makes a
difference, this would be a serious matter.
The
rapidity with which treatment can be inaugurated
after the onset of the
illness is by far the most important
factor therapeutically. Next in
importance ranks the quality
of the personality before the illness began. A
frank, open and
socially well-adjusted personality reacts better than
one
which has always been shy, shut off, awkward and autistic.
There are
probably a number of reasons for this. The autistic
personality may not have
always been so, but have become
so as the result of an early and unrecognised
schizophrenic
process, which -has perhaps become chronic, only to show
a
recent florid exacerbation. Further, restoration cannot at
its optimum
be to the same level in the defective as in the
thoroughly normal
personality. This is perhaps the principal
factor that militates against the
successful treatment of
schizophrenia in the intellectually
retarded.
Rapidity of onset is generally held to be a favourable
factor,
which would imply that in two schizophrenics in both of
whom the
illness was of three months' duration, the one in
whom it began in florid
form would have the advantage over
the other in whom it began gradually. This
may be because
in the latter the true point of onset would be set further
back ;
but it may also be because the more acute illness is more
easily
reversible.
The bodily physique has been found to be of
importance,
and the pyknic or athletic habitus is more favourab!e than
the
asthenic and the dysplastic. This is a very general
clinical
impression, and has recently been confirmed by
Freudenberg.
Freudenberg has also found that an abundance of "
process
symptoms," such as hallucinations, thought disorder,
primary
delusions, passivity feelings, etc., are unfavourable. A
history
of a previous attack with a full remission, is on the other
hand,
a favourable sign. It is also our impression that an
atypical
quality in the symptomatology is a sign of good omen.
These
favourable and unfavourable factors seem to act
cumulatively, and very
satisfactory results can be expected
from the patient who shows all of the
first and none of the
second, whereas if the opposite is true treatment is
hardly
worth while. In patients who fall between these two groups
the
results obtained will also be intermediate; there will not
be the same
frequency of complete success as in the most
favourable group, but
considerable improvement, sufficient
for social rehabilitation, will often be
obtained even where a
complete remission appears unattainable. It will be
seen that
the factors that favour a satisfactory response to insulin
are
also those clinically associated with a higher expectation
of
spontaneous remission; but this would be an inadequate
argument in
favour of a laissez-faire attitude. The tragedies of
neglected insulin
treatment in England are to-day a commonplace
to the psychiatrist of
experience; we have as yet
seen no tragedies from premature treatment
skilfully applied.
THE RISKS OF
TREATMENT
The risks of treatment are in
general less than the risks of
waiting for spontaneous remission to occur.
Massed figures
gathered in the United States give a mortality of 90 deaths
in
12,000 patients treated, of which about half were due to
hypoglycaemic
encephalopathy, which is thus seen to be the
most serious risk of treatment;
it is, on the other hand, a:n
avoidable risk and is the rarer the more
skilled the operator.
In this series there were also twelve deaths from heart
failure,
nine from aspiration pneumonia, seven from pneumonia
occurring
otherwise, some of which were probably also avoid-
able. The New York State
hospital figures show that there was
a higher mortality in the untreated than
in the treated
patients. It may be that patients with better physique
were
selected for treatment, and if so that could partly explain
the
result. It is also true that the patient's bodily health
rapidly
deteriorates. under an acute schizophrenic psychosis,
thereby laying him open
to a greater risk of tuberculosis and
intercurrent disease .han where the
process is cut short by
treatment. Twelve patients died of pulmonary
tuberculosis
in the control group, only one in the insulin treated group.
A
mortality of less than one per cent. cannot be considered a
reasonable
bar to treatment in the average patient; and the
risk of death or serious
damage to bodily health can be
neglected in all but the physically ill. Any
advanced degree
of cardiac disease is usually considered a contraindication
to
treatment, as are also Graves disease, diabetes, liver and
kidney
diseases causing marked impairment of function.
Treatment can be dangerous,
and is rarely successful, above the
age of forty-five.
Careful
investigations have shown that in patients with a
prolonged series of deep
comas there is sometimes a mild
degree of intellectual impairment the effect
is much smaller
than that also seen in patients of all kinds treated by
con-
vulsion therapy, which is far from great or constant. The
degree of
impairment has been of practical importance in
only a handful of patients
reported in the literature, and is in
any case not comparable with the
disability caused by the
disease itself. Mental impairment is of much greater
im-
portance after long irreversible coma, and a severe Korsakow
picture
can result from this. This improves somewhat as a
rule, but usually leaves a
greater or lesser degree of permanent
impairment. Its occurrence is the
principal reason why the
deliberate production of irreversible comas, which
often have
an immediate curative effect on the schizophrenic process,
has
not been extensively tried as a method of treatment, and
should remain
exclusively in the hands of treatment experts
of long experience. A minor but
still important reason why
treatment as early as possible is so desirable, is
that there is a
lesser necessity for repeated deep comas, with the
attendant
risk of irreversible coma.
THE TECHNIQUE OF
TREATMENT
We are indebted to the
Journai of Mental Science for permission to
include in this chapter the
illustration and some of the details of technique
from an article by Fraser
and Sargent 1940
The
beginner would be well advised, before starting this
treatment, to go for a
week or more if possible to a hospital
where it is done on a fair scale. The
technique cannot .be
learned from books alone, and some practical experience
is
necessary of the dangers that may be met with.
The following technique
here described mostly arises from
experience gained from 1937 onwards at the
Maudsley Hospital
in conjunction with Dr. Russell Fraser, and subsequently
in
an E.M.S. Neurological Unit where early cases could be
admitted and
treated under the conditions obtaining in a
general hospital.
Lack of the
best facilities should not prevent treatment
altogether; and the dangers of
treatment under adverse cir-
cumstances may have to be balanced against the
dangers of
delay. It is quite possible to carry out the insulin
treatment
of schizophrenia in a general ward, with the patient
screened
off during the coma period. Nevertheless where schizophrenics
are
going to be treated in any number a special insulin
treatment unit is very
desirable. Excited patients cannot be
easily handled in general wards, and
even quietly behaved
schizophrenics are likely to become noisy and difficult
during
hypoglycaemia. A fairly large room should be taken, in which
all
the patients it is proposed to treat at one time can be kept
economically
under observation: off this there should be
one or two side-rooms available
for the more restless and
noisy. These rooms will be kept at a warm
temperature, as
patients perspire profusely and often throw off their
bedclothes.
To staff the unit a well-trained team of nurses is
required,
of whom as many as possible should have both a general
and a
psychiatric training. Experience of medical and
surgical emergencies is very
valuable in the management of
this complicated method of treatment. A sister
should be
in charge, and on duty during the treatment period every
day.
Changes in staff from day to day mean that minor
alterations in the behaviour
of individual patients during
sopor and coma may be missed, to the danger of
the
patients: for behaviour varies widely from patient to patient
while
remaining very constant to the individual, and a nurse
who knows the patient
well can detect signs of danger Jhat
would not be at all noticeable to anyone
else. Every effort
should therefore be made to keep the team together, and
avoid
changes of more than one of the personnel at a time or at
less than
well-spaced intervals. The sister is of coutse the
most important of all; and
it will be her responsibility to
assemble and maintain the equipment so that
none is astray
at an emergency.
The patients also should be kept together
through the
greater part of the day. Their food intake at every meal
has
to be carefully supervised, and they themselves must be kept
under
supervision to prevent the occurrence of after-shocks
in the afternoon or
evening. If they go out in the afternoon,
it should be in the company of a
nurse supplied with glucose
to give to any of them who may suddenly develop a
recurrence
of hypoglycemic symptoms.
Apart from the usual ward apparatus
such as intravenous
syringes (1 to 20 c.c.), intravenous needles kept
freshly
sharpened and in perfect state, a variety of small basins,
swabs,
surgical spirit, etc., the following special equipment
is required:
blood-pressure apparatus, air-way, tongue-clips,
mouth gag for use in the
event of a fit (a rubber heel covered
in mackintosh or a dogs small rubber
bone are serviceable),
an emergency apparatus for giving 5 per cent. carbon
dioxide
in oxygen, ampoules of adrenalin, morphine, hyoscine, 10 per
cent.
calcium chloride, sodium amytal, atropine, coramine,
eucortone, nicotinic
acid, vit. B.1, and luminal (all suitable
for intravenous and intramuscular
use). The means of cutting
down on a vein should also be at hand.
On one
or two small portable trays are placed the means of
nasal interruption. The
nasal tubes selected should be stiff and
of fine bore, and should be
discarded when they get soft from
repeated boiling. On the same trays there
will be lubricating
oil, litmus paper and an aspiration syringe for sucking
out a
test sample of the stomach contents through the nasal tube.
The
container of 600 c.c. of 38 per cent. sugared tea (6.5 oz.
sugar to the pint)
is also on this tray. The tea should be
prepared before treatment starts in
the morning and kept till
needed in bulk in a large jug containing sufficient
for the
needs of all patients. This reservoir of sugared tea must be
kept
warm, for instance in a large thermos jug, and from it
the smaller
receptacles for individual trays can be filled just
before
interruption.
Another special tray or trolley holds the equipment for
an
emergency intravenous interruptionone or two syringes each
containing
20 c.c. of fresh sterile 83 per cent. glucose solution
and a sterilised bowl
from which they may be rapidly refilled.
Sealed bottles of 38 per cent.
glucose should also be at hand,
and only opened before the injection starts.
There should be
ample amounts of 5 per cent. glucose saline ready for
emer-
gency intravenous use, but it need not be specially
heated.
Sarganta and Fraser have adapted
for use in insulin therapy a
composite pressure apparatus which avoids the
necssity of having
to change syringes in giving large quantities of 33 per
cent glucose
or glucose salines intravenously, with the risk of losing one's
place in
the vein every time the change is made. From the illustration it
will
be seen that it is a simple pressure bottle attached to a syringe with
a
side-valve. The needle is inserted into the vein, and with the first part
of the 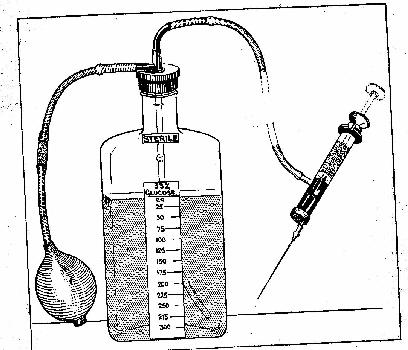
plunger, blood is sucked into the
syringe, thereby showing that the needle is
in position. Further withdrawal
of the plunger beyond the side-valve allows
the 33 per cent glucose solution
in the pressure bottle to flow freely through
the syringe into the vein.
Bottles of 5 per cent saline are kept in stock which
also fit the same
screwcap of the apparatus. If after the 33 per cent glucose
has been given, a
change to 5 per cent glucose or saline is required, this is
effected simply
by unscrewing one bottle and screwing on the other, pressure
being
re-established by more hand pumping. Through all this, the doctor's
attention
can be concentrated on the more important job of keeping the needle
in place
in the vein, a ticklish matter if the patient is excited and restless,
while
the nurse does the pumping and
changes the bottles if .necessary.
Emergency drugs such as
coramine can be injected into the rubber connection
between
the bottle and the side-valve syringe without further interference
with the veins.
For the avoidance of unnecessary risks, the closest
atten-
tion to record keeping is required. The quality of the records
will
often distinguish a good clinic from a careless one. Four
separate records
are recommended. There should be a tem-
perature chart, on which are
entered the temperature, pulse
and respiration rate daily at 6 a.m. and 9
p.m., the diet taken
(as full, half, or excess), any tube feed that may
have
had to be given, the daily insulin dose, duration of coma and
time
taken to awake after interruption. Any special com-
plication is marked by an
asterisk on the chart. The weight
recorded weekly or hi-weekly is also noted.
A space is left at
the side of the chart for entering the average coma dose
of
insulin and the maximum safe period of coma for that par-
ticular
patient, after these have been ascertained during the
treatment.
A
daily treatment chart is also kept. On it are shown half-
hourly records
of pulse and respiration rate during treatment,
the amount of sweating, the
amounts of insulin and glucose
given each day, the time of onset of sopor and
coma and the
time taken to come round after interruption. Details of
the
patients behaviour and neurological abnormalities in sopor
and coma
are also noted here.
In a conspicuous and convenient position in the ward
there
is a treatment board. On it are marked the times of onset
of
sopor and coma, the time when each patient is due to be in-
terrupted,
the time he is actually interrupted and the time
of his awakening. It is
filled in as these events occur by the
doctor and nurses. The important data
it provides can be read
at a glance from any part of the ward, and help to
prevent
delays and omissions when emergencies engage the attention
of the
staff too exclusively to one patient. It is also useful for
providing the
data of the more detailed and permanent records.
Lastly, there should be an
insulin dosage book, in which the
next days doses are entered at the end of
each mornings
work. It is for the information of the sister or nurse in
charge
when giving the insulin the next morning.
Before treatment is begun, it is
desirable to deal with any
septic foci that may be present, at least if of
gross degree and
fairly easily treated. There is evidence that insulin
resistance
is increased by even a mild infective process.
Great importance
should be placed on giving a correctly
balanced diet during treatment. If
possible, measured normal
meals should be prescribed and kept approximately
of the
same content each day. Excess of carbohydrates in the diet
enhances
the probability of after-shocks by increasing insulin
sensitivity. The aim
should be to have every patient on a
constant diet, a regular daily routine
and the same length of
coma each morning. When the metabolism is kept steady
in
this way, it is rare to get sudden changes in the response
to the
morning insulin or the occurrence of after-shock,
Furthermore, any ominous
irregularity in behaviour is
more likely to be noticed and reported. If the
diet taken is
inadequate tube-feeding must be resorted to. It must be
re-
membered that a morning dose of insulin may still be in process
of
absorption for eighteen hours after it has been injected.
Much of the
treatment devolves on the nurse, and on her
skill its success depends.
Provided she is well chosen, the
more responsibility she is given the better
the standard of
work she will attain. The sister and the senior nurses
should
be trained in all details of the technique, from the passing of
the
stomach-tube to the intravenous interruption, and they
should be able to
carry out these procedures with confidence.
They learn to judge for
themselves when the patient is going
too deep, or showing abnormal symptoms,
and to report to the
doctor in time. In an emergency they are taught to act
for
themselves, and may have to do so if complications arise in
several
patients at a time and the doctors whole attention
has to be concentrated on
only one. If the selected male and
female nursing staff are trained to a high
pitch of efficiency,
a greater number of patients can be treated than if the
doctor
has to undertake every routine procedure himself. A doctor
must
always be on call, but it is not necessary with a trained
staff for him to be
in the insulin room except during the
times of sopor and coma. If the nurses
have been especially
well selected and trained they can even be left to
handle the
early stages of sopor and light coma provided the doctor
can
get to the treatment ward within a minute of being
summoned.
We give full treatment on five days
a week. On the sixth
half-doses of insulin are given, and the seventh is a
rest day.
If time is short, however, full treatment can be
advantage-
ously given on six days a week. The commencing dose of
insulin
is usually 20 units at 7 a.m. given intramuscularly by
the nurse in charge,
with the patient fasting from 8 p.m. the
night before, and the dose is
increased by this amount each
day of full treatment until sopor occurs, when
progression of
dosage may be slower. When high doses of insulin have
been
reached without sopor, the jump may be 80 to 40 units each
morning
instead of 20 units. Once coma has been induced,
the insulin dose should be
adjusted until the minimum
satisfactory coma dose has been found. Neglect of
this
principle will lead to the occurrence of irreversible comas.
Insulin
sensitivity frequently increases during treatment,
and the regular daily dose
may eventually be stabilised at
half the amount that was necessary to produce
the first coma.
Furthermore, often enough the patient seems consciously
to
resist going into sopor or coma, and when he finally does
so a much
lower dose of insulin is needed to induce the same
state on subsequent
occasions. Sometimes sodium amytal
gr. 3 to 6 has been given by mouth at 7
a.m. when the insulin
is given. This may make the patient less restless and
enable
him to pass more smoothly into sopor. This dose of amytal
is not
enough to make the sleep induced by the drug indis-
tinguishable from the
hypoglycemic phenomena. Sometimes
very high doses of insulin fail to produce
conih at all. Then
the doses must be swung. On one day 240 units
should
be given, and then in rotation 40, 120 and 240 units. In this
way
insulin sensitivity may often be increased to the point
where a satisfactory
coma is induced. Insulin resistance up
to 600 units has, however, been
reported, and the phenomena
of insulin resistance are little understood. Some
patients, for
instance, may go into coma with as little as 40 units or
even
less.
There is much confusion about the correct use of the
word
coma". It is generally agreed that the length of time the
patient is
actually unconscious is the best index of the severity
of a period of
hypoglycemia. Yet in papers on technique
daily comas of two and a half hours are
recommended by
some, while others advocate only three-quarters of an
hour.
These discrepancies are due to differences in the meaning given
to
the word coma. The criteria of coma given by Kuppers
have been adopted in our
work. He differentiates the stages
of loss of consciousness into sopor or
pre-coma and true coma.
Because of individual variations it is generally
found that
reflexes, motor phenomena, and most other physical signs
cannot
be used as criteria of onset of either of these stages,
and reliance has to
be placed on tests for the presence or
absence of conscious or purposive
reactions.
The onset of sopor is usually indicated by the loss of a
normal
response to speech and impairment of orientation.
But testing will still
elicit Ssome confused but purposive re-
sponses. There may be some difficulty
in deciding the exact
time of onset of sopor from earlier degrees of
hypoglyc~mia.
This is not so important as to recognise when sopor
deepens
into coma. The onset of coma is distinguished by the loss of
all
purposive responses, simulating those of the conscious
patient, even on
careful testing. There should be no responses
from visual, auditory or
tactile stimuli. Painful stimuli may
still produce some movements, but these
are not directed
towards the stimulus., Tests should include raising
and
dropping the patients arm, trying to make his eyes follow
a moving
object, and giving a painful stimulus such as pressure
on the supraorbital
nerve. As coma supervenes the eyes may
still remain open and some
non-purposive movements persist,
but the absence of purposive response can
always be demon-
strated by testing. Some patients, while still in sopor
and
aware of the test stimuli, lose all initiative to respond. They
must
be distinguished from those in coma, and generally
painful stimuli will
reveal the difference.
THE SECOND
PHASE
The second phase of
treatment starts when the patient
begins to go into sopor. The regulation of
hypoglycaemia to
achieve the maximum degree of safety is best done by
con-
centrating on the duration of actual coma rather than of
sopor. But
very occasionally hypoglycaemia has become
"irreversible when the patient is
allowed to remain at the
stage of apparent sopor for a very long
tIme. As a precaution,
therefore, interruption is carried out after an hour
and a half
of sopor, if coma has not supervened.
When the patient has begun to
go into coma the length of
the coma period allowed is increased gradually
from five
minutes on the first day to what proves to be the maximum
safe
duration for the individual. Using the criteria given
above, the average
daily period is half an hour, with con-
siderable individual variations above
and below this figure.
The physician should not rely on rule of thumb, but
should
try to discover the safety limit for each patient. He may be
warned
that coma is getting too deep by the patient taking
over twenty minutes to
awake after the nasal feed. He should
be guided by this, or interrupt when
other signs of excessive
depth occur. As the patients physique improves with
treat-
ment, longer comas can be tolerated than initially; this will
be
indicated by changes in the depth of coma or alteration in
waking time.
Sometimes it may be desired to take the patient
particularly deep. If this is
done it is wise to interrupt
immediately afterwards by the intravenous route,
and not to
wait a further twenty minutes or less for the patient to
come
round after a nasal interruptionunless after thorough
testing this
has been found to be safe. A particularly severe
coma is also apt to cause an
increased susceptibility to the
next days insulin, and this must be
remembered if deep
comas are given. To prevent irreversible coma, a
shorter
coma is advised on the day following a deep coma, particularly
if
there have been signs of shock or delayed awakening. For
the general run of
patients, it is best to give a maximum safe
coma treatment, and to stick to
it each day until recovery is
manifest. Some patients, however, do well with
submaximal
comas, and others need dangerously deep comas to
achieve
results. This is why results vary from therapist to therapist,
and
success depends so much on his skill. With increas-
ing depth of coma comes
an added risk of irreversible
coma, and great skill is needed to handle this
emergency,
but the risk must be faced if it is necessary to the
patients
recovery.
Our remarks apply to comas
occurring at the end of the
third and the beginning of the fourth hours, and
are not
applicable to those beginning in the fifth hour. Margins
of
safety must necessarily
be loWer in the latter. The insulin
dosage should be so adjusted as to induce
coma about three
hours after injection.
SIGNS OF DANGER, EXCESSIVE
DEPTH AND EXHAUSTION
Signs of excessive depth call for
interruption at any stage
of coma. The peripheral circulation and blood
pressure are
valuable indicators of circulatory embarrassment, and
re-
peated examination of the finger tips is advisable. When the
blood
pressure falls below 100mm. or the peripheral circulation
becomes poor the
coma should usually be interrupted. A
falling blood pressure and a rising
pulse or respiration rate
should always be regarded as a danger sign,
especially if
combined with signs of failure of peripheral
circulation.
Interruption must be done in good time; the tube feed may
be
vomited or poorly absorbed, and when intravenous inter-
ruption is attempted
the veins may be found to be collapsed
and may then have to be cut down on.
If pulse irregularities
first appear during the later stages of coma and the
pulse drops
below 55, interruption is advisable. Earlier pulse
irregularities
before the onset of coma often subside with its onset,
and
should only require caution when they are frequent or persist
for over
half an hour. As a general rule, provided the blood
pressure remains above
100, the pulse volume is good and the
pulse between 70 and 100 per minute,
these patients may be
left for three-quarters of an hour before interruption.
Some
patients who start with extra-systoles in the initial stages
of
treatment lose them as treatment progresses.
Motor neurological signs
are of little help in determining
the onset of coma, but they are useful
indications of its depth.
In the earlier phase various types of movement may
appear;
they are clinically important only if they are excessive
and
produce exhaustion. Occasionally they may be the pre-
monitory signs
of an impending fit. The movements should
not be allowed to continue for over
an hour and a half or less
if the patient is becoming exhausted by them.
Premedication
with luminal gr. 1 to 2 or sodium amytal gr. 8 to 6 may help
to
diminish them or prevent their occurrence. If the jerking and
movements
are too great it is sometimes advisable to give
intravenous sodium amytal gr.
2 to 3.5 at the time to reduce them.
The drowsiness induced by such a
small dose of intravenous
amytal is easily distinguished from true coma and
may
enable the patient to pass through the restless phase
into
coma.
According to Mayer-Gross severe
hyperkinetic conditions,
restlessness and noisy excitement, can also be
controlled by
giving a part or the whole of the morning insulin dose
intra-
venously. This brings on the deeper and quieter stages of
coma more
quickly. One has to learn by trial in each case
how much of the total dose to
give intramuscularly early on,
and how much intravenously at a later stage in
the days
treatment.
In the deeper stages of coma
waves of extensor tonus
occur which are well seen in the arms as combined
extension
and pronation. They are really important, as they indicate
that
the safe limit of coma is being reached. But these move-
ments are often
precipitated or exaggerated by respiratory
embarrassment or circulatory
failure. If the air passages are
freed by inserting a Hewletts airway and
the extensor tonus
then subsides, coma may be allowed to continue. When
these
waves of extensor tonus are only spasmodic and the state of
the
circulation is satisfactory, coma may be continued for a
further fifteen
minutes before interruption. But to be on the
safe side it may be advisable
to interrupt intravenously at the
end of this time and not await the slower
operation of a nasal
feed. If the waves persist for longer than a minute, or
the
circulation is poor, immediate interruption should be
done.
Generalised tremor when the patient is not cold is another
important
sign of excessive depth and calls for early inter-
ruption. After going into
coma sometimes the patient
awakens spontaneously, generally after a period of
severe
spasmodic movements. If he is allowed to relapse into coma
agail
after this it should oniy be for half the normal length of
coma, or even
less, as this phenomenon may be the precursor
of an irreversible coma. The
condition of the reflexes is of
little help in giving warning of excessive
depth. More im-
portant is any change from the usual ueurological
pattern
seen during previous comas. If unconsciousness seems deeper
or the
neurological pattern different from the usual for that
particular patient,
and the circulation is poor, interruption
should be done as a precautionary
measure.
OTHER
COMPLICATIONS
Epileptic fits occur early or
late in the hypoglycaemic
period. The early fit occurs 45 to 100 minutes
after the start
of treatment and before the onset of coma. It is
generally
easy to manage. Often after it is over the patient wakes
up
spontaneously and can drink his sugared tea, or glucose can
be given
nasally or intravenously if he remains confused.
Fits occurring in late sopor
or during coma are more dangerous
and may be followed, especially in the case
of those occurring
in the later stages of coma, by delayed recovery or
severe
shock. Immediate intravenous interruption is necessary for
these
later fits. Sometimes absorption of sugar from the
stomach does not occur for
some hours afterwards, and
therefore further intravenous glucose may be
necessary in an
hours time, and even again later in the day. Fluids
are
valuable when signs of shock are present; up to 500 cc. of
5 per cent.
glucose saline may be given after an initial 250 cc.
of 33 per cent. glucose
intravenously. Late fits in the stage
of. coma probably indicate excessive
cerebral glycopenia,
and that is why they should be dealt with efficiently
and
rapidly.
Respiratory complications
occasionally arise from aspiration
of saliva during coma, because of increase
of salivation and
diminution of protective reflexes. In the later stages of
sopor
and during coma the patient is best turned on his side to
permit the
saliva to drool out of the mouth. Respiratory
stridor occurring in coma and
not due to blocking of the air
passages nor relieved by passage of an airway
calls for im-
mediate intravenous interruption as it may be a
dangerous
complication.
Vomiting after nasal interruption can often be
dealt with by
giving atropine gr .001 to .02 intramuscularly some
minutes
before the nasal feed. It is only a dangerous complication
when it
indicates a condition of shock. If it does, the treat-
ment of shock will be
required, i.e. intravenous glucose and,
if necessary, saline.
INTERRUPTION
In the lightest stages of
hypoglycemia the patient can, as
a rule, drink 600 c.c. of 33 per cent.
sugared tea (for preference
flavoured with lemon) at the end of
treatment. In sopor and
coma the same amount has to be given by means of a
nasal
tube. When the tube has been passed, gastric juice should
be
withdrawn and tested for acidity with litmus paper before
the sugar is poured
down the tube. When the gastric juice
is only weakly acid a teaspoonful of
salt is added in case
chloride deficiency is being caused by excessive
sweating.
When coma has been deep it is unwise to allow more than
twenty
minutes to elapse in waiting for the patient to come
round before giving
glucose intravenously. This time may
have to be shortened if coma remains
deep or other signs of
danger are present. When a skilful technique in the
pre-
servation of the veins and the use of the pressure bottle has
been
acquired, therapy may be conducted on the basis of a
routine intravenous
interruption. Longer and deeper comas
can then be given with greater safety.
The state of the veins
must be kept under observation and one or two
unharmed
veins should be always kept in reserve for use in emergency;
if
thrombosis has occurred in most of the conveniently placed
veins a return to
nasal interruptions is indicated. In inter-
ruption by the intravenous route
100 c.c. of 83 per cent.
glucose is generally sufficient, but up to 250 c.c.
may be given
with safety. The patient receives further sugar to drink
when
he awakes.
After the patient has come
round he may be given a light
breakfast. Lunch should be given about 1 p.m.,
tea at 4.30, and
another meal in the evening. The commonest time for
after
shocks is about four hours after interruption. If the patient
is not
taking proper meals additional glucose may be given
at this time as a
prophylactic.. But it has already been
pointed out that too great a
carbohydrate preponderance in
the diet is undesirable. Regular balanced
supervised meals
at the right times and a correct morning dose of insulin
are
the best prevention of after-shocks.
IRREVERSIBLE
COMA
This is a dangerous
complication in which unconsciousness
persists despite the giving of adequate
intravenous glucose. In
severe cases there are pronounced vascular shock,
hypertonus,
writhing movements, and the condition resembles one
of
anoxia. The milder cases
may merely show delayed local
recovery, such as monoplegia or aphasia or a
slight confusional
state of short duration. The severe case may involve days
of
unconsciousness, but with skilful handling death should be
avoided. The
pathology of the condition is unknown; but
treatment must be directed towards
facilitating the entry of
glucose into the brain cells, combating the
alkalosis and
anoxia, and restoration of the circulation to its
maximal
efficiency. We have seen great benefit from the giving of
large
amounts of intravenous salines in these cases. When the
patient does
not come round as he should with the intra-
venous administration of 100 c.c.
of 38 per cent, glucose, this
condition must be assumed to be present; and
before the
needle is withdrawn an additional 150 c.c. of 33 per
cent.
glucose should be immediately given. If the patient still has
not
come round, 10 to 80 c.c. of 10 per cent. calcium chloride,
2 to 4 c.c. of
coramine, 20 mgms. of vitamin B. 1, and 500 to
1000 c.c. of 5 per cent,
glucose in saline should be given intra-
venously, starting as soon as
possible. The end of the bed
should be raised, 5 per cent. CO2 in oxygen is
given to the
patient and warmth applied, including hot-water bottles,
as
for shock. After these measures the degree of shock should
be
subsiding, and the rectal temperature will generally rise,
but the patient is
often still very restless. An injection of
morphia and hyoscine is useful for
allaying this.
An hour after the first
injection a second injection of
250 c.c. of 33 per cent. glucose, together
with a further 500 c.c.
of saline, should be given if necessary. If treatment
has been
prompt and efficient, by this time the danger of acute
collapse
is usually past; but the patient may not recover
consciousness
for many hours or even days. Often absorption from
the
stomach starts again very slowly, and further intravenous
glucose has
to be given later in the day, as insulin is still being
absorbed from the
morning Thjection. A stomach-tube
should be passed when first aid measures
have been completed,
and four-hourly nasal feeds of glucose are given. If
these are
not being absorbed they are withdrawn every four hours and
fresh
glucose substituted until stomach absorption restarts.
Each time the previous
feed is found unabsorbed, or has been
vomited, 500 c.c. of 5 per cent,
glucose in saline should be
given intravenously. In very severe cases in
which it does not
appear
probable that the patient will come round tor a long
time a vein should be
cut down on and a continuous glucose
saline drip started. Blood transfusions
may be given alternat-
ing with the saline drip. Eucortone has been
recommended.
Nicotinic acid mgms. 100 four-hourly may also be given
during
the period of unconsciousness by the intravenous
route via the continuous
drip. The patients strength must
be maintained by intravenous feeding till
stomach absorption
restarts.
With prompt treatment recovery
from this condition gener-
ally takes place in the first twenty-four hours;
but a period of
unconsciousness lasting six days has been seen, when
the
doctor had failed to institute emergency measures immediately.
After
long periods of unconsciousness very marked impair-
ment of intellectual
functions will be seen, but a surprising
degree of recovery from this will
occur in succeeding weeks
and months. Following short-lived irreversible
comas some
dramatic improvements in schizophrenic symptomatology
have been
recorded. If, with effective measures, the patient
has emerged rapidly from
irreversible coma, the fact that the
complication has occurred does not imply
that treatment
should be abandoned. It may be started again in three
or
four days time, but thereafter the comas must be kept much
shorter. On
several occasions we have known treatment,
started again under these
circumstances, to proceed without
further mischance to a successful
conclusion.
CLINICAL CHANGES PRODUCED BY
TREATMENT
In patients who are going to
react well to the treatment it
will generally be found that after the first
few comas, wakening
from coma leads to an hour or two of a considerably
improved
mental state. Sometimes in the early case improvement
occurs
without the coma stage having been reached. The
most prominent change is a
great improvement in rapport and
the affective attitude. For a time the
patient regards the
doctor and the nurses in a much warmer and more
friendly
manner, suspicion is for the moment in abeyance, and there
is
often a considerable degree of insight into the delusions, feel-
ings
of unreality, etc. After this short interval, however, the
patient sinks back
into his old state, and remains in it for the
rest of the day. Patients who are excited,
agitated or panicky
are often much improved in this respect for a longer
period of
time. As the days of treatment succeed one another
the
beneficial change lasts longer, and the state into which the
patient
relapses becomes less hind less severe, until gradually
the improvement is
maximal. In the most fortunate patients
this may occur with astonishing
rapidity, less than a fortnight
of intensive therapy sufficing to bring about
what appears to
be a complete cure.
In order to judge whether the
maximum amount of benefit
has been gained it is necessary to have a very
thorough
knowledge of the patients symptoms and clinical state
before
beginning treatment. As improvement takes place delusions
and other
morbid ideas which have hitherto been concealed
may be brought to the light
of day, and give a false im-
pression to the naive that the state is becoming
more acute.
A very careful clinical examination should be repeated
when
the termination of treatment is being considered; and treat-
ment
should not be stopped if there are any signs of activity
of the disease,
unless it is thought hopeless to proceed any
further. By this it is not
meant that the patient must have
full insight into the symptoms of the past,
but that there
should not still be hallucinations occurring, or feelings
of
influence or passivity, etc.
Furthermore, it is probably
desirable to continue a more
modified form of insulin treatment until the
patient has
regained the physique that is normal and healthy for him.
It
is quite possible that relapse is more likely, even when there
is complete
restoration of mental normality, if a really good
state of bodily health has
not been regained. Mental im-
provement and physical improvement usually go
side by side,
but one may lag a bit behind the other. If the patient
regains
his normal weight and physical state, and retains his
mental
symptoms unaltered, it is a bad sign, and it is usually not
worth
proceeding much further. Most favourable cases respond to
treatment
within two months. Sometimes recovery seems to
occur two to four weeks after
treatment has been completed.
If no change has been brought about in three
months, and
every therapeutic trick has been tried, it is unlikely that
there
will be a favourable outcome,
USE OF CONVULSIVE THERAPY WITH INSULIN
Although convulsive therapy
is no method of treatment of
the schizophrenic psychosis itself, it can often
play an adjuvant
part, and be particularly useful for dealing with
individual
symptoms. Depression in schizophrenia, as in
basically
different disorders, is often much improved by a few
electrical
fits; and their use before the treatment proper is begun
may
allow the patient to be more easily treated, and may, if neces-
sary,
permit the physician to get a clearer perception of how
much schizophrenic
disturbance there is actually present.
Depression in schizophrenia is
a secondary symptom,
possibly partly psychogenic in origin, possibly partly a
result
of the metabolic changes that are having a total effect on
the
patients health; but the intensity of the affective change
may
obscure the realisation of the more fundamental and
ominous symptoms. The
hypothymia, lassitude and anergia,
which are more directly related to the
schizophrenic process
may also clear up under the influence of a few
convulsions,
which are more likely to be required for that purpose after
the
termination of insulin treatment than before it has begun.
Catatonic stupor usually yields
to convulsive therapy, but
sometimes passes into a catatonic
excitement.
Convulsions should then be used if there is doubt of
the
diagnosis, or if the catatonic state interferes with the
practical
details of insulin therapy, e.g. in the intake of an
adequate
diet, Qr if the condition fails to respond fairly rapidly
to
insulin and a depressive component is suspected. The insulin
treatment
will itself be nearly always required to establish
ground gained by
convulsive therapy, and to prevent the
possibility of rapid relapse. Insulin
will also remedy sympl~ms
of thought disorder untouched by convulsions. There
is
some evidence that a few convulsions may be of benefit
during the
course of insulin treatment, for instance when the
patient has started to
improve, but has failed to maintain
improvement. Where the two treatments are
combined they
should be given separately and not on the same day. The
role
of convulsive therapy in schizophrenia is therefore a
supplementary but
important one; the improvements claimed
in the past from convulsions alone
have mostly been symp-
tomatic ones without significance for the course of
the
disease, or have proved temporary. Some of the few apparent
cures may
well have occurred in what were fundamentally
depressive illnesses, with a
schizoid colouring derived from the
structure of the personality. The highest
recovery rate in
any large and varied group of cases .initiaiiy diagnosed
as
schizophrenia will be achieved when insulin and convulsion
therapy are
skilfully combined in differing proportions in
each case, based on the actual
symptomatology shown.
PSYCHOTHERAPY
In our view the time has passed
when one can legitimately
treat schizophrenia by non-physical methods alone,
and the
claims that are from time to time made of the necessity
of
combining psychotherapy with insulin treatment seem to
be exaggerated.
Many patients make an uninterrupted
recovery under insulin treatment without
any special psycho-
therapeutic handling whatever. The apparent
psychological
precipitants of a schizophrenic illness are frequently
found
when the insight gained into the illness is fairly complete to
have
been not part causes of the illness but the earliest signs
of its onset. The
type of psychotherapy that is most required
with the schizophrenic patient is
of a kind that might be found
valuable after any grave physical illness. Once
he is re-
covered the patient has to return to the outside world and
try
to manage his own affairs without the constant advice of the
doctor;
it will often help if the way is made a little smoother
for him. While the
disease is in active progress it is hopeless
to try to influence the
patients ways of thinking; but it is not
so hopeless when the fundamental
thought disorder has been
abolished, and there are only a few fragmentary
delusional
beliefs, suspicions or foci of apprehension which are left
over
as relics from the past.
It is probably beneficial to
get into contact with the patient
during the best half hour or so of the day
immediately on
wakening after treatment, and to give him then the
im-
pression of friendly assistance, even though, as is probable,
any
influence one can exert on his morbid ideas is of the most
trifling duration.
As soon as he is well enough he should
be kept fully occupied in the
afternoon with occupation
therapy, gardening, games, walks, visits to the
cinema, and
so on. When
recovery has occurred the possibilities of
explanation and reassurance are
much more favourable.
The patient will probably have a very clear memory for
a
time of his many morbid experiences, and will be anxious to
get some
explanation for them. Reassurance will also often
be required on the subject
of relapse. It should not be
concealed from the patient that relapse may
occur, but he
should be told that the prospects of treatment need be
no
worse, should a relapse occur, than they have been with his
first
illness, and that if he only seeks advice in the early days
of such a
recurrence, they are bright indeed; he should, of
course, on the other hand,
be encouraged not to worry about
himself, nor to keep forever a finger on the
pulse of his mind.
FOLLOW-UP
When recovery has occurred it
is advisable to discharge
the patient from hospital as rapidly as possible.
Return to
the normal environment, and an abbreviated recollection of
the
hospital atmosphere will aid the patient in the recovery of
his
self-confidence and powers of adaptation. But it is ad-
visable to keep an
eye on the patient in an out-patient clinic
fairly regularly for a month or
so, and then it is wise to ask for
three-monthly attendances for another
year. If there is the
slightest sign of any relapse it should be promptly
dealt with,
and though a relapse may occur at any time up to many
years
later, it is most likely to occur fairly soon.
| Click on these buttons to visit our journals | ||||||||
| Psychiatry On-Line |
Dentistry On-Line |
Vet On-Line |
Chest
Medicine On-Line |
GP On-Line |
Pharmacy On-Line |
Anaesthesia On-Line |
Medicine On-Line |
Family Medical Practice On-Line |
All pages copyright ©Priory Lodge Education Ltd 1994-2003.